
Is this Philadelphia businessman peddling quackery? Or is the profit-driven American medical establishment trying to ignore Jim Caplan's miracle treatment?
“I knew my foot would have to be amputated, but I didn't think it would be this soon,” says Adaria Young, 31, of Philadelphia. She has been a diabetic since she was 4. Because diabetes reduces the feeling of paint, Young didn't realize she had been walking around for several days with a thumbtack stuck in her right foot. The foot became infected, the infection spread to her bone, and her foot was amputated in September.
“At first it was frustrating, but it was something I have to live with,” Young says. I have a 6-year-old, and I knew I had to be strong for him.”
So far, her left foot seems to be OK. “I have to be really careful, she says. “I have to keep something on my feet at all times, and when I take a shower I have to check between my toes [for infection or drainage]. So far, I've been really lucky.”
According to the Centers for Disease Control in Atlanta, Young is among an estimated 13 million Americans with diabetes, though only half of all diabetics have been diagnosed. Diabetic circulatory disorders like Young's contributed to more than 162,000 deaths in 1990, making it the seventh leading cause of death that year, according to CDC records.
In 1994, the National Institutes of Health (NIH) earmarked $301.3 million for diabetes research. It is among this country's most broadly studied diseases, with 17 different institutes at NIH funding research on everything from blood-sugar levels to peripheral-nerve destruction. Despite all the researchers have learned, American doctors still are poorly equipped to handle diabetic gangrene and infections that lead to amputations.
Meanwhile, for decades, doctors in Germany have been healing diabetic wounds with ozone, a very strong form of oxygen applied directly to the wound. But the German technique is not available in the United States, partly because bringing it to market could cost tens of millions of dollars—or more—and no company could recoup that kind of an investment with a simple, unpatentable chemical.
“It feels like somebody's stabbing you with a knife,” says Dorothy Simmons Hardy of Philadelphia. “It’s constant, sharp, achy pain. It never lets up. The pain is real severe, and it's real constant.”
Simmons Hardy is one of about 72,000 people in the United States who suffer from sickle cell anemia. When the oxygen level in her blood drops too low, her blood cannot flow normally. The pain usually hits her legs, but sometimes she has arm and stomach pain. Frequent hospital stays make it hard for her to hold a job. She almost died twice during pregnancy because of sickle-cell complications, including a blood clot on the lung.
NIH spends about $70 million a year to study sickle cell anemia. Statistically, relatively few people suffer from this disease compared to other ailments. But American scientists say a disproportionate amount of energy is focused on sickle cell because they consider it a great medical challenge: In 1954, Linus Pauling won a Nobel prize for identifying sickle cell anemia as a genetic defect, making it the first genetic defect found in humans.
For years, NIH has funded research into lowering the percentage of sickle hemoglobin in-the blood. Drugs such as hydroxyurea and butyrate are being tested at Children's Hospital in Philadelphia and throughout the country. But now those drugs are on the back burner, and the hottest sickle-cell research is in gene therapy, the idea that technology could permanently alter people's cell structures to cure diseases. Dr. Junius Adams, a health-scientist administrator at NIH in Bethesda, Md., says gene therapy is “really the only thing we've got going that has potential to cure sickle-cell disease.”
Some scientists predict gene therapy could become reality within-five years; others say it's closer to 40 years, maybe more. Meanwhile, Philadelphia businessman and ozone proponent Jim Caplan has convinced doctors in Cuba to treat sickle cell anemia with ozone, much as the Germans are treating diabetics.
At the moment, the best American doctors can do is put their sickle-cell patients on antibiotics to stave off infections while the blood circulation is limited, and give them painkillers to help them ride out the painful crises. But Cuban doctors have documented that in their research, the use of ozone cut the length and the severity of painful episodes in half. So far NIH grant reviewers have opted not to put research money toward this treatment.
As his immune system has steadily fallen apart, one Philadelphia man says he has lost 40 pounds in four months from AIDS diarrhea, what doctors call “AIDS wasting.”
“It's a severe problem,” says this resident of Betak, a Philadelphia nursing home for AIDS patients. The man, who asked not to be named, is resigned to his unrelenting diarrhea. “It doesn't really ever go away. They try to control it with medicines. It works a little, but it's an ongoing thing... It has a tendency to drain you, make you very tired.”
At the end of 1993, there were 54,000 AIDS patients across the United States who had AIDS wasting. NIH has set aside $1.3 billion for AIDS research in 1995. At least $4.6 million a year is reserved specifically to study AIDS wasting, which hit 14 percent of Philadelphia AIDS patients in the last year.
Some vaccines are being tested on AIDS patients in the United States, but most of the NIH-funded research focuses on the basic science of how HIV works, what causes the virus and how it spreads.
Meanwhile, a San Francisco researcher conducted a study in which four out of five AIDS-wasting patients found relief with ozone therapy. A virologist in New York found that ozone was able to attack HIV-infected cells in the laboratory, but healthy cells were not affected. Neither of them has been able to get NIH funding to continue their ozone research.
Too little research, too little profit
What if scientists came up with a stunning medical breakthrough that might be able to help doctors treat a variety of diseases, but nobody had the chance to get rich from it?
Though Young, Simmons Hardy and the AIDS patient all suffer from different maladies, there are American researchers who say there is reason to believe that each of them could be helped with the same incredibly cheap, incredibly simple drug: enriched oxygen, a.k.a. ozone.
Ozone is used to treat patients in other countries, but not in the States. Here, in the country with the highest medical standards in the world, it hardly been tested. The same costly, lengthy, bureaucratic approval process that protects Americans from potentially hazardous drugs also is keeping Americans from lifesaving therapies.
This is a story about a potential cure that no one has been able to research thoroughly in the United States, in part because trying to sell ozone would be like trying to sell air—there wouldn’t be enough private profit in it.
This is a story about the American medical establishment considering itself more scientific and ethical than the medical systems of other countries – and, as a result, looking skeptically at what doctors in the rest of the world are doing.
Finally, this is a story about an idealistic man who wanted to do good in the world by introducing German successes to the American medical establishment. He found that isn’t so easy.
Some say the American medical system is working as it should end that if ozone turns out to be an ultimate therapy, someday it will get its do. Others say ozone research is held back because it’s an unconventional approach competing with more conventional experimental treatments, and a system that bases its agendas on long years of preliminary laboratory testing. Because there has been a little American research to determine whether Germany’s medical results are valid, there’s no jumping-off point for the theory in the United States.
“It was a fresh idea,” Rosemont resident Jim Caplan says. “I just thought, ‘my gosh, you open the window for them and they’re going to fly.’ They didn’t fly.”
Ozone: Dangerous and wonderful
Ozone (O3) is a form of oxygen (O2) produced when an electric spark or ultraviolet light is passed through air or oxygen. When you flip a light switch and see a spark, you've created a small amount ozone. “Any electrical discharge cross in the air will create certain amount of ozone,” says Bob Steeves, a lawyer and pharmacist at the Food and Drug Administration's Office of Orphan Products Development in Rockville, Md. Ozone easily reverts to regular oxygen again.
Ozone has both very bad and very good properties. It’s good in the sky, bad in the lungs.
The ozone layer in the earth's atmosphere protects us from harmful ultraviolet radiation, which causes skin cancer and other problems. That’s why environmentalists and public-health organizations are so concerned about automobile exhaust fumes combining with the sun’s rays to burn holes in the ozone layer.
Ozone also is a severe lung toxin. People working with it must be careful not to release it into the air they breathe.
“Ozone can do many, many things. It's amazing,” says Toshio Asakura, an M.D. and Ph.D. at Children’s Hospital in Philadelphia, as well as a professor at the University of Pennsylvania. “Ozone is also a very dangerous chemical.”
Ozone “pretty much kills every known microbial thing out there,” says Lt. Col. and Dr. Donald Skillman, chief of infectious diseases at Fitzsimons Army Medical Center in Denver. It causes free radicals, chemicals that can kill. It can lead to cancer. “Like anything else, it's toxic in high concentrations.”
Ozone is very unstable: The third oxygen atom likes to break off and attach to other things, including bacteria and viruses that do not grow in an oxygen environment. The human immunodeficiency virus (HIV) for example, dies when exposed to air. Ozone is the most powerful oxidant known.
In Japan, ozone has been bubbled into fish tanks with amazing results, Asakura says. He doesn't know how it works, but “the fish grow so big compared to the sibling fishes. This is a fact.”
Germans began using ozone as early as World War II for cleaning and disinfecting wounds, but it was difficult to handle because oxygen with just 5 percent ozone would corrode rubber and various metals. The development of modern plastics made it possible for Germans to resume ozone therapy in the 1960s.
Since then, German doctors have been working with ozone to treat a variety of problems. They’ve had especially good results treating infections and wounds, like diabetic ulcers. Sometimes they draw blood from the patient, bubble ozone into that blood and then re-infuse the oxygen-rich blood into the patient. Sometimes they apply ozone to the skin in a closed container, like a plastic boot. Sometimes they give ozone enemas. In each scenario, oxygen atoms break off from the ozone and bond to oxygen-poor blood or stubborn infections.
Ozone kills bacteria and fungi as well as improving circulation, according to German doctors S. Rilling and R. Viebahn, authors of The Use of Ozone in Medicine. They write that ozone stimulates the body's ability to carry crucial, life-giving oxygen to the body's tissues.
American doctors know that oxygen helps tissues heal, but they're not always sure how to get oxygen to where it's needed. Simply breathing oxygen doesn't seem to do much good. Neither does putting people in pressure chambers with oxygen. “I think in theory, ozone has potential to be helpful in eradicating many types of infections,” Skillman says. “It could be used in many different fields.”
Starting with strawberries
For one thing, ozone is useful for shipping strawberries. When Jim Caplan was 17 years old, he and his father started installing ozone generators on railcars carrying strawberries from California and Texas to the East Coast. The ozone, O3, would quickly decompose into more stable oxygen molecules, O2. The extra oxygen atoms would attach themselves to mold spores and protect the delicate fruit.
As a teenager, Caplan was intrigued by ozone. In the 33 years since, Caplan has spent much of his spare time reading about, thinking about and talking about ozone.
For six years now, Caplan has been pushing and cajoling American doctors and researchers to consider ozone as a treatment for sickle cell disease. His crusade, reminiscent of the parents’ chase for an ADL cure in Lorenzo’s Oil, hasn't made him a lot of friends in the American medical establishment. “Oh God, not that guy. Ozone Enemas himself,” came the response from Adams at NIH.
“Mr. Ozone Enemas” actually is a comfortable businessman, husband and father to four children living in a white house in the suburbs. He has a bachelor’s degree in economics from Penn State. As a National Science Foundation fellow, he studied at the London School of Economics and Yale.
Even as a child growing up in suburban Philadelphia, Jim Caplan was something of an independent spirit who liked intellectual challenges.
“Growing up as an only child, you learn to fight your own battles,” he says. Without brothers or sisters, “there’s no one to confer with.”
He liked playing sports. He read a lot. When he was about 12, he read a Clarence Darrow biography and decided to become an attorney. That thought was short-lived.
“I didn't like the idea that you could end up defending an argument you didn't believe in,” he says. “I didn’t want to be a lawyer after that.” I wanted to understand everything about people,” he says. “I was interested in the labor movement. I was interested in how people lived, how you had poor people and rich people, and what made the system what it was.”
So Caplan studied economics to become a businessman, and he continued thinking about ozone. Then while he was living in Tegernsee, Germany, from 1969 to 1972, Caplan found himself at a Waldfest drinking beer with Dr. Josef Issels, a German cancer specialist who tried to bring about remissions in terminal patients. Issels told Caplan of his efforts to build up the immune system and reduce the spread of cancer with ozone.
Meanwhile, Caplan read about the work of Dr. Ottokar Freiherr van Rokitansky, chief surgeon at a Vienna hospital. Rokitansky reportedly used ozone to decrease the number of gangrene-related amputations by 40 percent. In 1983, Caplan met Rokitansky at an ozone conference in Washington, D.C., where the researcher was reporting on his work with ozone to treat circulatory problems.
In 1987, Caplan became CEO of his father’s Philadelphia business, Capp, Inc. The business primarily makes temperature controls for melting things like metals, plastics, pharmaceuticals and Hershey's chocolate. Caplan says the work sharpens his determination to find answers to technical problems. “You can't leave a company like DuPont up in the air,” he says, “or they won't do business with you anymore.”
In 1988, he saw one of his employees, Dorothy Simmons Hardy, trying to recover from a sickle-cell crisis. “At 2 o’clock in the afternoon I would see her with her head on her desk terribly fatigued,” Caplan says.
He wanted to help. He turned to a general medical text, Boyd's Pathology, and looked up sickle cell anemia. The book described red blood cells that lose their shape and elasticity when the blood's oxygen partial-pressure falls below 45 millimeters of mercury.
Oxygen pressure. Caplan remembered the strawberries. He remembered the doctors in Germany. Then he wondered: Why not use German ozone techniques to treat sickle-cell crises? If Germany can do it, why not the United States?
Closed doors at Children’s
“I reviewed the material Mr. Caplan sent me,” says Dr. Alan Schechter, a sickle-cell specialist and chief of the Laboratory of Chemical Biology in NIH's National Institute of Diabetes and Digestive and Kidney Diseases in Bethesda. “I was very impressed. The data looked very nice.”
“He’s right,” Schechter says. “If you could increase the partial pressure of oxygen, it would probably have a beneficial therapeutic effect [on sickle-cell patients]. I think it’s an interesting idea.”
Schechter suggested that Caplan take his idea to Children’s Hospital in Philadelphia, because Asakura is the person in the United States with the technology best able to measure the sickling of cells. Ironically, Caplan says he already tried to interest Children's.

Caplan says he first took the concept to Children’s, which receives $1.5 million a year from NIH as well as large private grants specifically to study sickle cell anemia. It has 22 sickle-cell studies going at the moment.
“I wanted them to join me and do the scientific research [on ozone therapy] in the United States,” Caplan says.
Caplan says he left an ozone generator and other equipment at Children's, and that he spoke every week with Asakura for two years. “I think Asakura was very interested in the possibilities here,” Caplan says. He says he hosted Asakura, his wife and other Children's staffers in his home to witness German doctors using ozone therapy. Asakura says he is “very interested” in studying the effects of ozone on sickle cell anemia, and that he remembers the hospital being approached by someone to study ozone. He says he can't remember who it was, but that it definitely wasn’t Caplan. “The hospital rejected the company because their interest is not the research, but the name of our hospital,” Asakura says, “This hospital decided that it is inappropriate that I conduct the research for the company.”
“[Children's] Hospital is very interested in any good research,” Asakura says. But Children's doesn't want him to accept research money from a for-profit company because there could be pressure to come up with certain findings, Asakura says. However, “I may [research ozone] in the future, when I have time and money.”
If Asakura can't remember Caplan by name, his supervisor certainly does.
“We just could not be pushed or coerced into an area of research we have no preparation for,” says Dr. Kwaku Ohene-Frempong, who heads up Children’s Sickle Cell Center.
“Ozone kills bacteria,” he says. “It will also supply a lot of oxygen to tissues that need to be repaired.” However, he adds, “medicine, or science, doesn't just run in fits and starts. You have to develop some scientific basis for something.” He points to acupuncture, the ancient-Chinese therapy that ever-so-slowly is gaining credibility in the United States. It takes time for the momentum and scientific paperwork to build up, Frempong says. “If I propose an ozone study to my institutional review board, they will think I'm crazy.”
Cutting the pain in half
After months of trying to interest American doctors, Caplan attended a 1989 ozone conference in New York. A delegation of Cuban scientists was reporting on their use of ozone to treat retinitis pigmentosa, a progressive retina disease that leads to blindness. Caplan mentioned sickle cell to them.
Cuban doctors Sylvia Menendez, Manuel Gomez and E. Espinosa were intrigued. Perhaps they could use a therapy they already were using safely, but for a new purpose. Statistically, sickle cell anemia strikes about 1 percent of all blacks—which is a significant number of people in a country that is more than half black. Caplan sent Gomez his notes.
At the National Center for Scientific Research and the Institute of Hematology and Immunology, both in Havana, the Cuban doctors started their research with animals to prove the ozone-enema treatment wasn't toxic. By May 1990, they already had conducted clinical trials with more than 100 sickle-cell patients.
The complex system of capillaries in the colon was able to pick up the oxygen and help the sickled blood cells flow more smoothly. The doctors reported that ozone helped patients resolve their sickle-cell crises in half the time, and that patients treated with ozone suffered fewer recurrences in the six-months afterward. (Their findings are published in the January 1995 issue of the Townsend Letter for Doctors, which calls itself “an informal letter magazine for doctors communicating with doctors.”) By November 1990, the Cuban Minister of Health approved ozone as a treatment for sickle cell anemia.
As Caplan figures it, the Cuban doctors who conducted the sickle-cell research are “wonderful caring human beings” who work 12 hours a day, six days a week. “They seem to be extremely dedicated to patient care.”
American doctors also want to improve patients’ lives, but it's harder for them, Caplan says. American doctors have to fight for their positions at hospitals, they have to plan their studies around grant money available if they work at research institutions, and they have to watch every step for fear of a lawsuit.
Cuban doctors don’t go through what our doctors go through,” Caplan says. “They can really practice medicine.”
Caplan presented a paper on Cuba’s ozone successes at the 18th annual meeting of the National Association for Sickle Cell Disease, held in May 1993 at Children's Hospital in Philadelphia. More than 100 caregivers were present, but not one doctor showed interest.
Several medical experts told the Welcomat they dismiss evidence from Cuba because they see it as a troubled Third World country without so much as a free press.
A tortoise among hares
It isn't easy to get the American medical establishment to pay attention to the work of doctors in other countries.
When American researchers hear of foreign data, “they tend to say ‘Who are these people? Are they running a monkey-gland clinic?’” says Art Caplan, director of the Center for Bioethics at Penn.
“The fact that [a therapy] is used In Europe doesn't really imply that it really is valuable,” says Schechter at NIH.
Realistically, the research findings might be less accurate outside the U.S. because, in most countries, researchers are allowed to try experimental treatments on people without double blind studies. In a double blind study, neither patient nor doctor knows who’s getting the drug and who's getting a placebo. Typically, patients could improve from a treatment simply because they expect to.
Other countries also are more willing to allow human experimentation without preliminary tests in test tubes and on animals, American researchers say. Plus, researchers in other countries don’t face the same significant studies to demonstrate a treatment is effective. When American pharmaceutical companies have an idea, they often start their research in Europe. By going overseas, drug companies can evaluate a drug faster and put it on the market there long before it hits the States, if it ever does.
“Their [European] procedures are much easier, so it takes less time,” says Mark Grayson, a spokesperson for the Pharmaceutical Research and Manufacturers of America. “The drug agencies aren't quite as intrusive, and they move much quicker than our FDA.”
Schechter and other researchers are quick to point out that Americans don’t want a drug that could be harmful to, say, one patient in 50. It seems odd to talk about researching a toxic cure. But German doctors seem to be able to use ozone without killing people, points out Art Caplan. To study the effects ozone on people, American researchers first would have to prove that it can be delivered without hurting people—which would be redundant when it's already being used safely in Europe, Art Caplan says.
Unfortunately, Americans “don’t have a way for systematically incorporating safety findings” from other countries, he says.
Perhaps worse yet, ozone's reputation in the U.S. suffers from people outside the medical profession who make claims before they have the scientific data. Certain people have offered ozone to desperate AIDS patients as a cure-all without the research to back their promises, Poiesz says. “If a concept gets associated with that, sometimes it's hard to break out of that cache of illegitimacy.”
Many American researchers, people who like to know the microscopic scientific steps within the overall process, are befuddled by ozone. It isn't completely understood.
“If you look at the studies that are done by the Cubans, it looks like they have major effects on their patients,” says Frans Kuypers, a Ph.D. research scientist who has studied ozone at the Sickle Cell Center at Children's Hospital in Oakland, Calif. But “none of those [Cuban] studies clearly defines why it is effective.”
Test anxiety
The people who think ozone has potential therapeutic benefits are among the first to say ozone should be scrutinized with big, scientific American tests. They just want those tests to be done.
Because so many people have promoted the use of ozone, “it deserves some legitimate study to say does this stuff have a potential or not, just to put it to rest,” says Dr. Bernard Poiesz, a virologist who has studied the effect of ozone on the HIV virus at the State University of New York at Syracuse. “There's a lot of clinicians that are using it for all kinds of things.”
Here in the United States, Dr. Michael Carpendale of San Francisco has been studying the potential uses of ozone for 15 years. He says all of his research has confirmed what German doctors have been saying about ozone’s benefits.
Carpendale studied five AIDS patients who had suffered from AIDS diarrhea for an average of 38 weeks. He found that four of the five patients improved after ozone-enema treatments. The results were published in 1993 in the Journal of Clinical Gastroenterology.” Although it was only five patients, it was very meticulously studied, very rigid,” Carpendale says. “We thought once we published that, that it would be easy to get funding for a proper study with 50 patients or 60 patients.”
A large study would be relatively expensive—$500,000 or so—because repeated lab tests would have to be done to track the treatment progress, Carpendale says. But “ozone isn't expensive in itself. It's just the-price of oxygen, and that's very cheap.”
Carpendale got some Veteran's Administration research money 10 years ago, and later he got some private funding that he stretched over two years, but he hasn't been able to catch the eye of NIH review committees. As he sees it, that's because ozone has no credibility in the “official party line” of conventional American medicine.
“It’s very hard to take that,” Carpendale says. “The thing is, I wouldn't mind if there were one good scientific study done to say ‘Look, it doesn't work.’”
Double blind “is certainly the right way to go,” Carpendale says. “But to put something down which they haven't done any tests on...”
“AIDS diarrhea is such a bad disease to have. To die of it is really very hard. But you really need to ask someone who’s more dispassionate than I am.”
At State University of New York, Poiesz has been frustrated, too.
In his study, he found that ozone could be used for “almost seemingly complete destruction” of HIV without affecting blood protein. It’s too early to jump to conclusions, he says, but the HIV infected cells were more vulnerable to ozone than healthy cells. This raises the possibility that AIDS patients could be treated with ozone.
His study also showed that a system to sterilize human plasma with ozone could be safe for handlers, he says. He thinks that theoretically, ozone could protect medical staff and patients from HIV and other viruses that have not yet been identified. The results were published in 1991 in Blood, the leading medical journal on blood and blood diseases.
Poiesz collaborated with Medizone, a New York company that hopes to get approval to use ozone to decontaminate blood products as well as treat viral diseases, including hepatitis B, herpes and HIV. Medizone International has worked with the Italian Scientific Society for Ozone Oxygen Therapy (ISSOT) on clinical trials at the University of Naples. If the process is approved, Medizone has patent rights to the process in the United States, Canada, Japan, Hong Kong and other countries.
Poiesz is interested in doing more ozone studies, but his research hospital can’t afford it. Medizone president Joe Latino has tried to find additional funding, but he hasn't gotten very far. NIH generally funds just 15 percent of research proposals, and this idea wasn't among them” The government deemed it not worthy of funding,” Poiesz says. He says there was a bias among certain project reviewers that ozone wouldn’t be very useful. “They just didn't think it had a priority.”
“What I really think we know about [ozone] is somewhere between nothing and not much,” Penn's Art Caplan says. “'What bothers me is that people aren't trying to push hard to get it tested” in the U.S.
A matter of money
American scientists spend many years studying individual steps in the basic science long before actual human beings are introduced to the equation. Then the clinical trials go on for years. Schechter has spent the last 10 years at NIH studying three drugs to try to increase fetal hemoglobin in the blood of sickle-cell patients. “It's very slow going.” he says, “We probably will not know the answers for three or four years” Historically, maybe one in 100 people who advocate an offbeat approach to medicine will turn out to have something important,” Schechter says. Unfortunately, nobody knows which Wonka bar has the golden ticket.
“I can tell you that there are 25 or 50 other types of compounds that people are advocating for sickle-cell therapy,” he says, adding that of 20 to 30 sickle-cell proposals in the ‘70s, “virtually none” are considered viable today.
At least half a dozen companies have potential sickle-cell drugs in the pipeline right now, he says. “They’re having the same type of frustration. What Mr. Caplan is experiencing with ozone is not unique.”
Realistically, researchers say, choices must be made.
“There are always many more important questions that can't get answered for lack of funds,” says Dr. David Asch, a senior fellow at the Leonard Davis Institute of Health Economics, University of Pennsylvania. Getting federal research money is a matter of convincing people that an idea has merit, he says. “You can’t test everything. I don't know if sucking on truck tires will cure cancer, but my guess is it won’t.”
Scientists know that oxygen can make sickled cells normal again, but ozone studies would have to progress from test tube studies to animal studies and then to human studies, says Frempong at Children's Hospital. “You can't jump over all those steps and just say, ‘I’m going to test this on humans.’ You can't just have a hunch and test it.” All this research takes money, and most of the money for research in this country comes from private industry. The pharmaceutical industry spends more than $13 billion a year on research—far more than the $700 million NIH allocates for studies, Grayson says.
Some of the proposals never pan out. On average, pharmaceutical companies spend $359 million per drug to get FDA approval, Grayson says. As a result, drug companies spend their research dollar “where they feel they’ve got a real breakthrough. You don't setup to do something somebody else is already doing.”
Financially, it doesn't make sense for drug companies to pump research money into ozone because drug companies are for-profit businesses. Ozone is a naturally occurring compound that can’t be patented...
The FDA realized that these financial realities and its strict regulation limit research into potentially useful drugs. So the agency set up an orphan drug designation to encourage research on diseases that affect 200,000 or fewer people in the United States.
The orphan drug program provides $9 million in grants each year, tax credits on research done, and a seven-year exclusive license if the process is approved by the FDA for that particular disease. Jim Caplan has orphan-drug designation for ozone to treat sickle cell anemia. If the process is approved, he would own the patent on the delivery process in sickle-cell cases for seven years. He says he hasn't even applied for orphan-drug research funding yet because he doesn't have the American scientists to conduct ozone research on sickle cell anemia.
An outsider looking in
Jim Caplan says he's frustrated. He doesn’t feel he's being taken seriously because he doesn't have “the right pedigree,” a medical degree. People from outside the medical world can be seen as the equivalent of snake-oil peddlers with “the latest-bottle of feel-good·stuff,” Art Caplan says.
But it's also hard for people within the system, Schechter points out. As Poiesz puts it, a businessman suggesting a medical idea is like a doctor trying to get a bill through Congress. He says he’s not surprised Caplan, an outsider to the medical establishment, has met with such resistance.
“Oftentimes, they get pretty chilly receptions,” Art Caplan agrees.
Always there are people who like to make money,” says Asakura at Children's Hospital. He says he would not be willing to join forces with a business that would sell ozone generators. “For pure science I am interested.”
“I wonder if they ever asked people like Frempong and Asakura how much Children's Hospital makes on sickle cell anemia,” Jim Caplan says. He says that if he were interested in profits, he wouldn't have devoted about 15 percent of his business week for years on end to an idea that might never see the light of day.
“I've gone all over the world and pursued this thing,” he says. “My whole motivation was to establish this mode of thinking and treatment. There are many other areas where I can make a profit.”
Improving lives
If a large, wealthy pharmaceutical company were steering ozone through the testing process, perhaps it would have a better shot. But the fact remains that pharmaceuticals would have no reason to take on a product as simple as ozone. As soon as the seven-year protection period ends, says Whitmore at the FDA, “29 companies are pumping it out in New Jersey.”
Jim Caplan doesn't care. “So you've got competition,” he says, “So you make a better product.” The real issue, he says, is the number of people whose lives might be improved with this cheap and simple process that needs to be tested.”
I grew up playing an awful lot of athletics. I like to win. If I think I'm right, I will persevere,” Jim Caplan says. He's trying to get as many people on his team as he can. There are people out there who will fight the fight. You just have to find them.” Even if he gets a seven-year ozone delivery patent for sickle-cell treatment, Jim Caplan believes he could not make nearly as much money from ozone therapy as the American health system could save if it were approved. Take the use of ozone to prevent diabetic amputations, for instance. He clicks some conservative numbers into his adding machine: “If you had 50,000 amputations a year and you reduced it by 35 percent, that would be... let's say the operation is $15,000, conservatively, with a stay in the hospital and the rehabilitation afterwards is another $15,000...”
Let's see... 17,500 people at $30,000 a head...
“That would be a savings of $525 million in this society.”
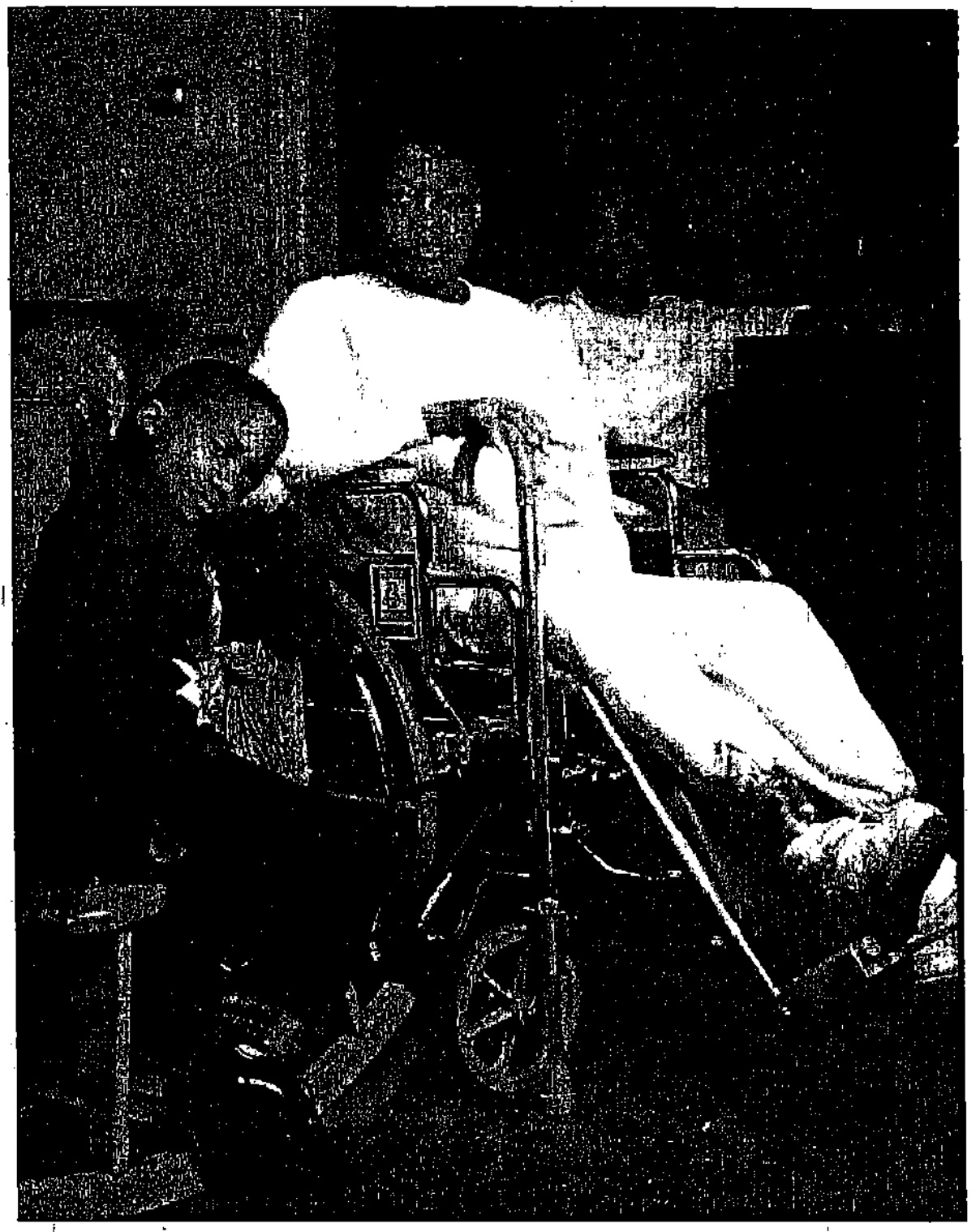
That's every single year. And that’s beyond the humanitarian side of things. In May l990, Jim Caplan saw a young Cuban woman lying on a treatment bench. “I came into the ward, and she was actually being treated for the ulcers on her leg,” he says. With repeated ozone treatments, he says her sores were going away.
“I was introduced as the man from the United States who introduced the ozone/ oxygen treatment-to Cuba,” Jim Caplan says. “The gal’s eyes lit up... [Through an interpreter] she said, ‘You know, all my life I've had these ulcers on my legs. I’ve never been able to go to the beach, I've never been able to wear a dress.
“She hugged me, and tears came to her eyes, and tears came to my eyes,” Jim Caplan says. “It was an extremely moving experience. It just makes you want to fight it through.”